
PART 1.1
The risk of smallpox was accepted as just an unfortunate part of life. Getting sick was a person’s fate. But in the late 1700s, Dr. Edward Jenner saw things differently and applied a “cause and effect” mindset. After years of observation, he was convinced that having cowpox protected people from contracting smallpox.

PART 1.2
In the early days of HIV/AIDS, AIDS was a mysterious disease. The cause of AIDS was unknown, and many blamed it on the most marginalized groups. But, without knowing that the disease was caused by a virus, it was easy to stigmatize, isolate and blame affected groups. The early approach towards understanding AIDS focused on who was getting infected, rather than the cause and effect of the disease. Epidemiologists saw that AIDS was affecting hemophiliacs, heroin addicts, homosexuals, and Haitians (the 4Hs of HIV) which biased the way people viewed the disease and the populations it first impacted. Infection did not seem to follow logic.

PART 1.3
Too many people were dying from automobile crashes on highways. But people considered these crashes to be “accidents,” or acts of fate for which we could not know the cause. They argued that if we could not know the cause, we could not prevent them. People were not thinking of cause and effect.

PART 2.1
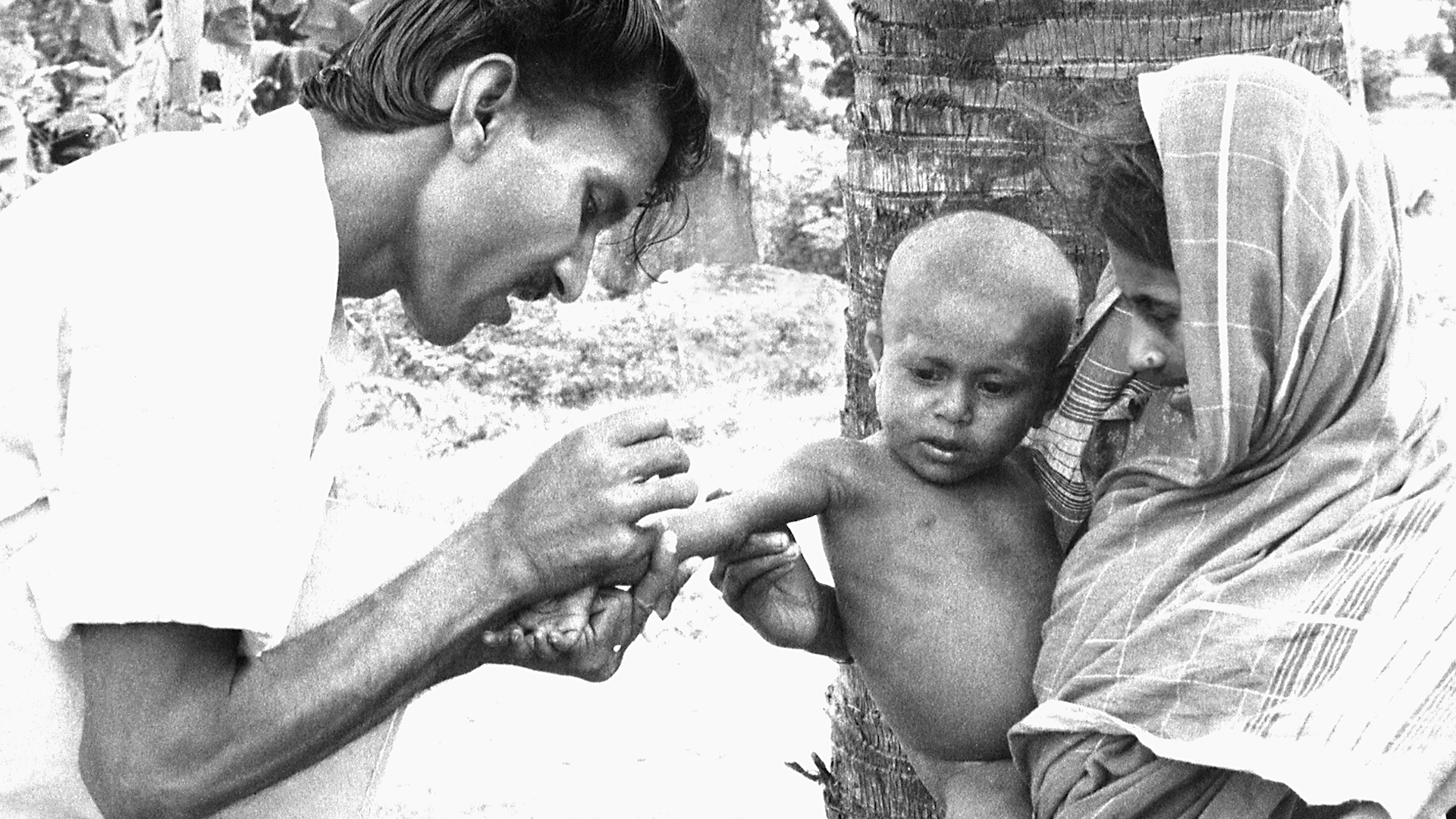
To apply the surveillance and containment strategy, it was necessary to know where the smallpox virus was, which villages had active cases of smallpox. The struggle against smallpox could not be won without knowing where the enemy was and what it was doing. But India did not have accurate surveillance data. Many villages with active cases had not been reported.

PART 2.2
While Guinea worm was widespread in Nigeria and Ghana, the leaders thought Guinea worm impacted only a small number of people and for this reason they were not motivated to do anything to solve the problem. But what government leaders thought were a few hundred cases turned out to be over 650,000 cases.


PART 4.1
Mass vaccination was the tried-and-true approach to smallpox eradication. Mass vaccination success was measured by the percentage of the population that was vaccinated, in order to achieve herd immunity. Most countries, WHO and other multilateral organizations were committed to this approach and operationally tied the goals to this strategic approach.

PART 4.3
When HIV first became prominent as a mysterious disease, people had many theories of how it was spread, almost all of them focused on the “immoral and drug-fueled” sexual activities of highly stigmatized groups. They not only held very strong views but they were absolutely certain that they were right. But the public, politicians and scientists were all challenged to rethink their ideas of spread when confronted by reports that the disease could be transmitted by infusing clotting factors from a donor to a patient with hemophilia.

PART 5.2
The polio eradication program relied on strong surveillance efforts to inform vaccination efforts. Surveillance teams worldwide constantly searched for cases in which people had limbs that could not be moved and just hung limply, or cases of “flaccid paralysis.”When they found these cases, they would target vaccination to those regions. This was a very effective strategy when polio was widespread, because almost every case of flaccid paralysis was caused by polio. As vaccination coverage increased, cases of paralytic polio plummeted. As cases of flaccid paralysis began to disappear, polio was declared eliminated from many countries and regions. But in many areas polio persisted.

PART 5.3
Infants were dying in rural health centers because they had complications that couldn't be dealt with in those hospitals. Doctors thought that a way to address this would be to transfer them to a larger hospital with more neonatal capacity. But, when the transfer solution was tried, it turned out that more infants were dying. Lives were not being saved. Babies continued to die because the transportation to the secondary or tertiary facilities took so long. The infants could not survive the trip.

PART 5.4
Gun violence takes an extraordinary toll on individuals, families, and communities in the United States. But the NRA has been successful in working through Congress to make sure that much of the critical data for assessing the problem, and finding interventions that work, is not collected, maintained, or made available.

PART 6.1
In the early 1960s, India accounted for nearly 60 percent of the reported smallpox cases in the world. The Indian government had launched the National Smallpox Eradication Program which focused on mass vaccination. By 1966, the Indian government reported approximately 60 million primary vaccinations. Mass vaccination campaigns had become part of the culture, and there was wide trust in this singular approach. However, the number of smallpox cases in India was increasing and India needed a new strategy.
PART 8.1
In 1973 India had thousands of cases of smallpox. For a while they were reporting one thousand new cases every day. Leaders of the eradication effort wanted to solicit help from WHO and bring in physicians, epidemiologists and health worker volunteers from other countries to supplement the Indian teams. But the Minister of Health for India felt that India had plenty of health workers and volunteers to do the job and said that people from other countries were not needed. The Minister's support for the smallpox effort was essential, so the team had to convince him to support bringing in workers from other countries without being critical of the great resources India already had.

PART 8.3
In February 2016, the World Health Organization declared the Zika virus outbreak a Public Health Emergency of International Concern. The Latin America and Caribbean (LAC) region was the most affected with more than 700,000 cases reported. In response to the outbreak, the U.S. Government allocated a portion of the funds remaining from the previous Ebola outbreak response to the LAC region. But money was not enough. The region lacked the public health and laboratory infrastructure for disease surveillance, contact tracing, and diagnostics, and needed to quickly build a workforce to respond and prevent future outbreaks.

PART 9.1
An effective vaccine for preventing smallpox had been discovered and tested by 1796. And by the 1970’s widespread vaccination resulted in most people in rich countries being vaccinated and almost completely protected. Smallpox was actually eliminated from developed countries in the 1970s. But the burden of smallpox was inequitably distributed. People in some poor countries remained vulnerable and faced high risks of mortality from smallpox. It was within the poorest communities that smallpox was spread.