
PART 1.2
In the early days of HIV/AIDS, AIDS was a mysterious disease. The cause of AIDS was unknown, and many blamed it on the most marginalized groups. But, without knowing that the disease was caused by a virus, it was easy to stigmatize, isolate and blame affected groups. The early approach towards understanding AIDS focused on who was getting infected, rather than the cause and effect of the disease. Epidemiologists saw that AIDS was affecting hemophiliacs, heroin addicts, homosexuals, and Haitians (the 4Hs of HIV) which biased the way people viewed the disease and the populations it first impacted. Infection did not seem to follow logic.

PART 1.3
Too many people were dying from automobile crashes on highways. But people considered these crashes to be “accidents,” or acts of fate for which we could not know the cause. They argued that if we could not know the cause, we could not prevent them. People were not thinking of cause and effect.


PART 3.1
Implementing the smallpox surveillance and containment strategy required massive resources, commitment, and coordination. But moving from a traditional strategy, used for over a century and a half with clearly defined roles for every participant, to a new strategy simply seemed too labor intensive and impossible. This required mobilizing and coordinating hundreds of thousands of implementers with a gradual increase in the number of people involved.

PART 3.2
Because of the experience with immunization and the successful eradication of smallpox, Dr. Jonas Salk, and Robert McNamara, past World Bank president, asked, “Why can’t the world be vaccinated the way the United States is?” There were good vaccines but poor global coverage. But the major agencies responsible for childhood immunizations were competing rather than collaborating and the immunization level was stuck at 20%.

PART 5.4
Gun violence takes an extraordinary toll on individuals, families, and communities in the United States. But the NRA has been successful in working through Congress to make sure that much of the critical data for assessing the problem, and finding interventions that work, is not collected, maintained, or made available.

PART 6.1
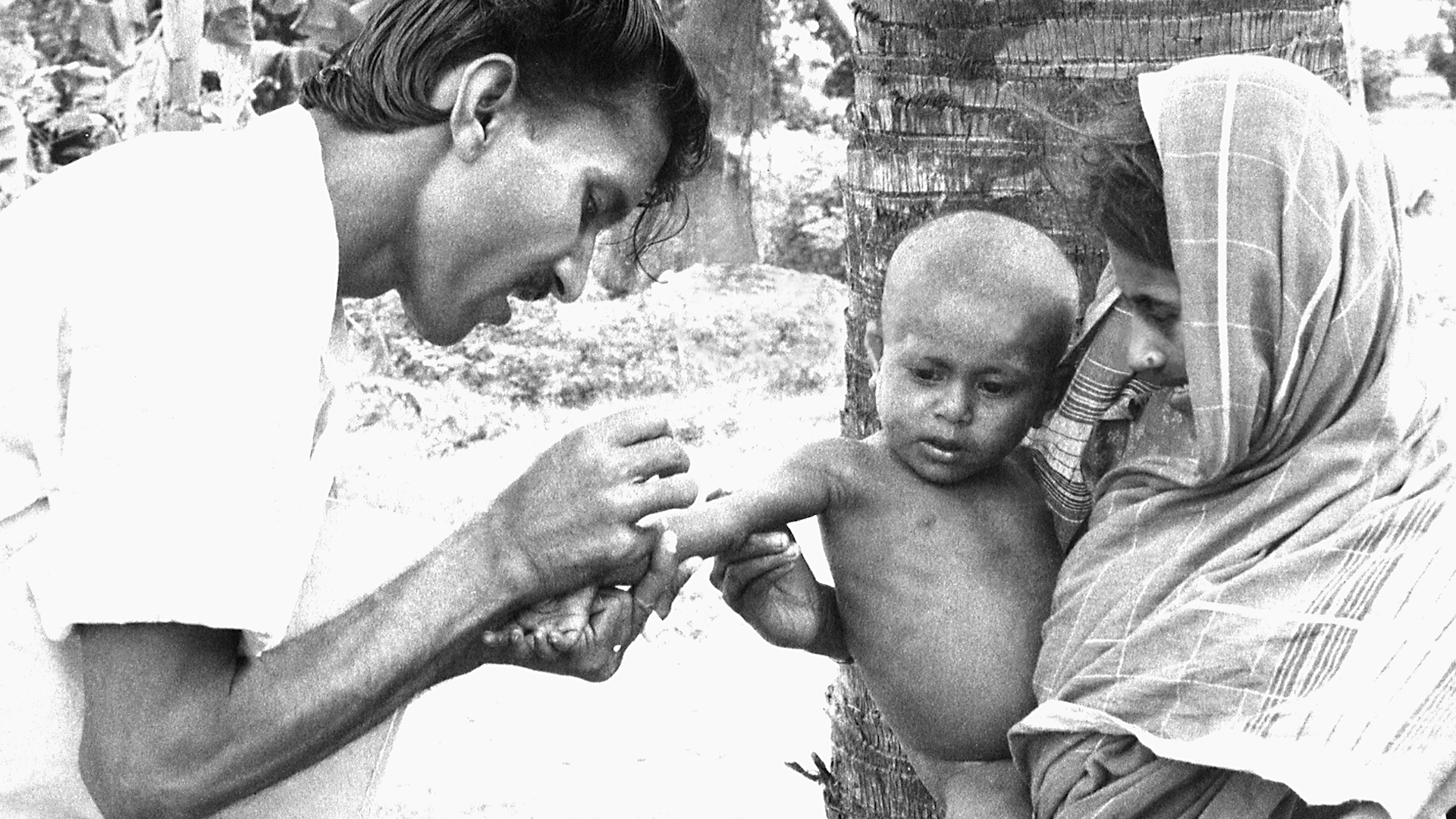
In the early 1960s, India accounted for nearly 60 percent of the reported smallpox cases in the world. The Indian government had launched the National Smallpox Eradication Program which focused on mass vaccination. By 1966, the Indian government reported approximately 60 million primary vaccinations. Mass vaccination campaigns had become part of the culture, and there was wide trust in this singular approach. However, the number of smallpox cases in India was increasing and India needed a new strategy.

PART 6.3
Gun violence research sought ways to prevent unnecessary gun deaths, disabilities, and anxiety. Many gun owners opposed research by the CDC on gun violence prevention because they believed that the goal of the research was to take their guns away. But the rise of mass school shootings led to a change in perspective because everyone was concerned about the safety of their children.

PART 8.1
In 1973 India had thousands of cases of smallpox. For a while they were reporting one thousand new cases every day. Leaders of the eradication effort wanted to solicit help from WHO and bring in physicians, epidemiologists and health worker volunteers from other countries to supplement the Indian teams. But the Minister of Health for India felt that India had plenty of health workers and volunteers to do the job and said that people from other countries were not needed. The Minister's support for the smallpox effort was essential, so the team had to convince him to support bringing in workers from other countries without being critical of the great resources India already had.

PART 8.3
In February 2016, the World Health Organization declared the Zika virus outbreak a Public Health Emergency of International Concern. The Latin America and Caribbean (LAC) region was the most affected with more than 700,000 cases reported. In response to the outbreak, the U.S. Government allocated a portion of the funds remaining from the previous Ebola outbreak response to the LAC region. But money was not enough. The region lacked the public health and laboratory infrastructure for disease surveillance, contact tracing, and diagnostics, and needed to quickly build a workforce to respond and prevent future outbreaks.

PART 9.2
Partners in Health (PIH) is a non-profit global health organization established by Paul Farmer, Jim Kim, and three colleagues to bring health care to the poorest people in low-income countries. PIH believed that these people deserve healthcare that was as good as the healthcare that rich people in the most advanced countries received. They found that poor people living in a shanty town outside of Lima, Peru had very high rates of multidrug-resistant tuberculosis (MDRTB), a disease that was notoriously hard to treat.

PART 9.3
There are medicines that could save the lives of the 500,000 children who die from malaria each year. Most of these children live in the low-income countries of Sub-Saharan Africa. Novartis manufactures the drug, artemisinin-based combination therapy, that is the standard of care for the treatment of P. falciparum malaria, the most deadly form of the disease. Although the global health community has for a long time been skeptical and wary of the private sector where profit was the driving force, Novartis happened to have a CEO who came from the field of global health and was inspired by the vision of global health equity. But neither these malaria-endemic countries nor WHO could afford to purchase commercially the amounts of this drug needed to treat the children who were at risk.