
PART 3.2
Because of the experience with immunization and the successful eradication of smallpox, Dr. Jonas Salk, and Robert McNamara, past World Bank president, asked, “Why can’t the world be vaccinated the way the United States is?” There were good vaccines but poor global coverage. But the major agencies responsible for childhood immunizations were competing rather than collaborating and the immunization level was stuck at 20%.

PART 4.3
When HIV first became prominent as a mysterious disease, people had many theories of how it was spread, almost all of them focused on the “immoral and drug-fueled” sexual activities of highly stigmatized groups. They not only held very strong views but they were absolutely certain that they were right. But the public, politicians and scientists were all challenged to rethink their ideas of spread when confronted by reports that the disease could be transmitted by infusing clotting factors from a donor to a patient with hemophilia.

PART 4.4
In the early 2000’s WHO had adopted the ambitious goal of getting 3 million people on antiretroviral medicines by 2005. But some people thought this was too ambitious a goal and that it could never be achieved. Leaders were afraid of making a mistake and being wrong, so they were hesitant to act until they were certain they could achieve their goal. Yet waiting would cause costly delays as the disease raged on, and prevent otherwise ambitious and very important programs from making progress.
PART 7.1
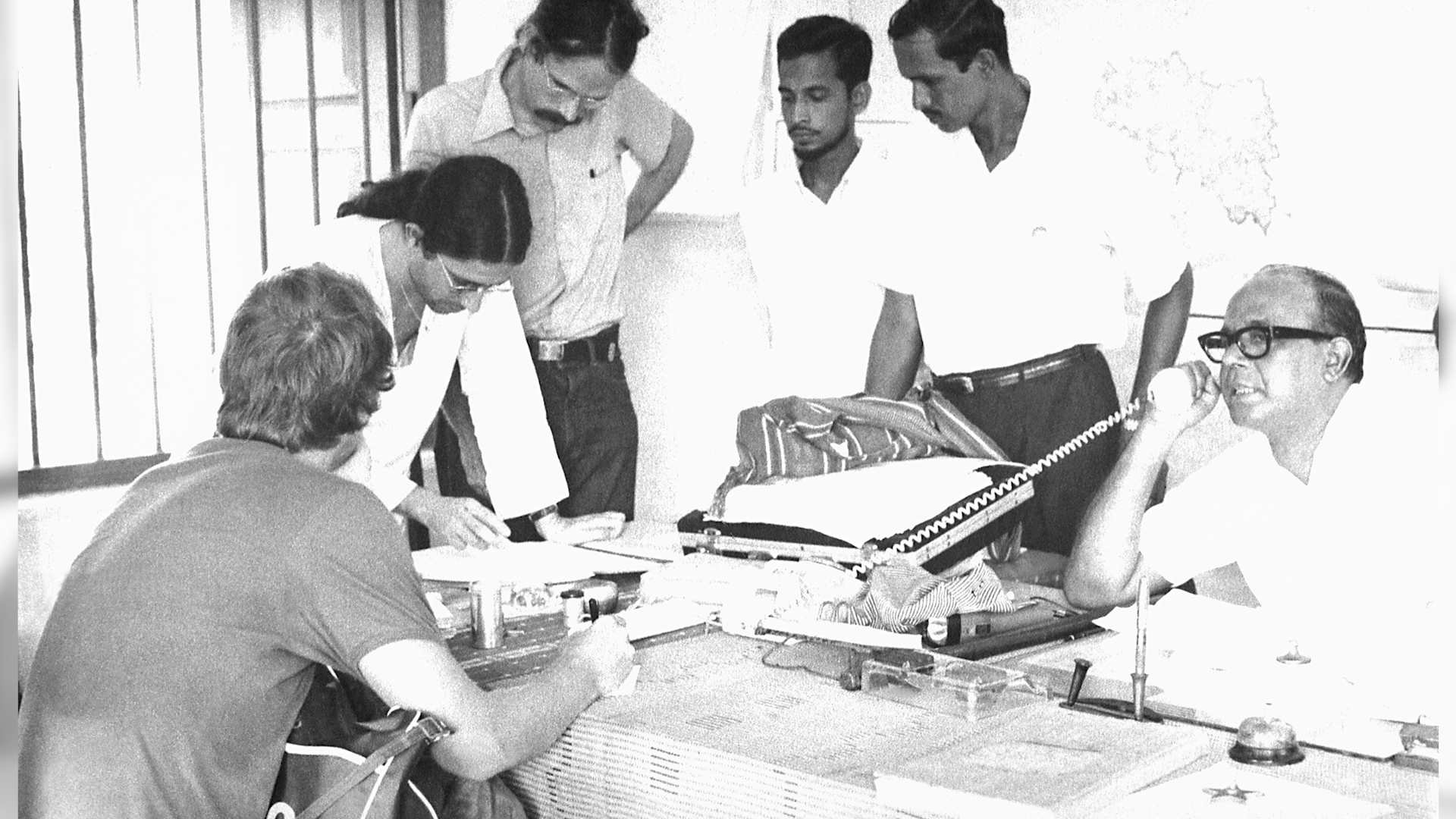
In early 1974, smallpox outbreaks were appearing in areas of India that had been smallpox-free for months. After a week of plotting the epidemic with pushpins on hand-drawn maps, a pattern emerged. Each outbreak began with a working-age young man who had returned home to his village. These cases were “importations.” The young men had come from—or traveled through—the bordering state of Bihar. Cases were originating in Tatanagar, the company town of the corporate behemoth, Tata Companies. Tatanagar, a city in the state of Bihar, had no centralized government, and no public health structure in place.

PART 9.3
There are medicines that could save the lives of the 500,000 children who die from malaria each year. Most of these children live in the low-income countries of Sub-Saharan Africa. Novartis manufactures the drug, artemisinin-based combination therapy, that is the standard of care for the treatment of P. falciparum malaria, the most deadly form of the disease. Although the global health community has for a long time been skeptical and wary of the private sector where profit was the driving force, Novartis happened to have a CEO who came from the field of global health and was inspired by the vision of global health equity. But neither these malaria-endemic countries nor WHO could afford to purchase commercially the amounts of this drug needed to treat the children who were at risk.